Join Us
Login
Home
About Us
About US
History of BISI
Society
Council
BISI Memorandum
BISI Memorandum Annexure Dec 2022
Membership
Membership Form
Member Directory
Education
Teaching Cases
2026
2023
2022
2021
2020
2019
2017
2016
Submit a Case
Fellowship
Dr Kakarla Subba Rao Travel Fellowship Grant
FNB Fellowships
Other Institute Fellowships
Certification Exam
Guidelines
Best Practice
Introduction
Algorithm for Breast Imaging
Mammography
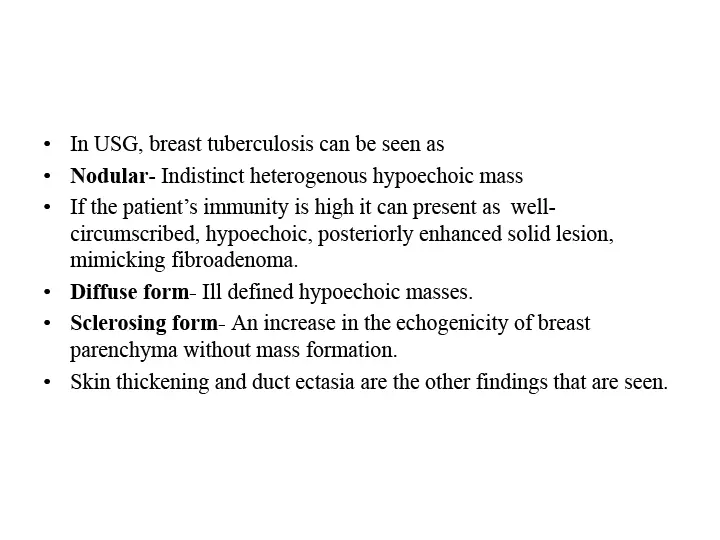
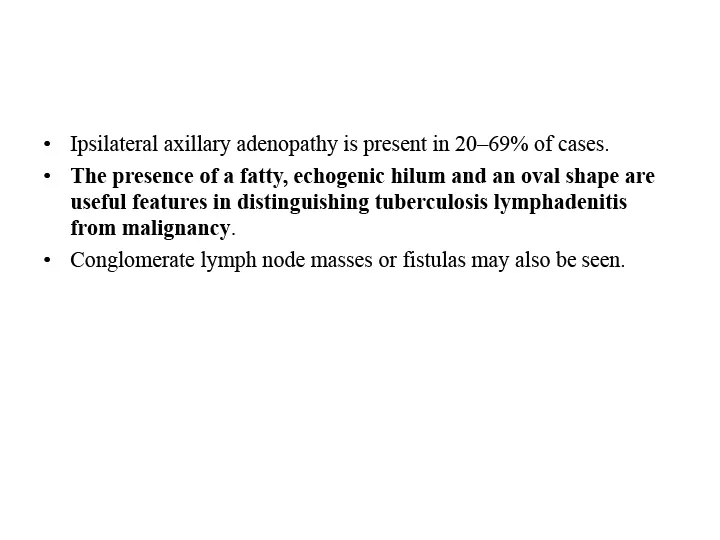
Breast Ultrasound
Breast MRI
Image Guided Breast Biopsy
Quality Assurance
Introduction Guidelines
USG guidelines
MRI Guidelines
MAMMO Guidelines
Events
BISI Endorsement
Upcoming Events
Social Events
BISICON
MID TERM CME
Society Endorsed Events
Newsletter
2019
2020
2022
2023
Ijbi
Public
Breast Self Examination
Breast Cancer Awareness
Mammography
Breast Ultrasound
MRI Breast
Breast Biopsy
Dense Breast
Contact
January 2026
We wish to bring many good things to life.
Home
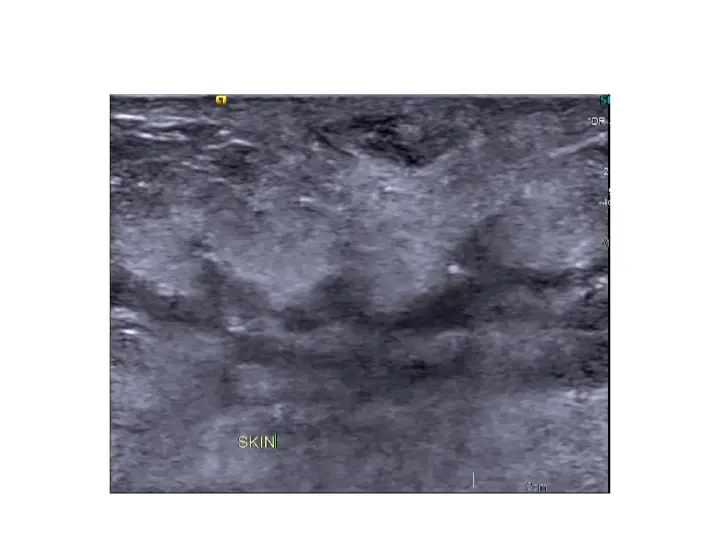
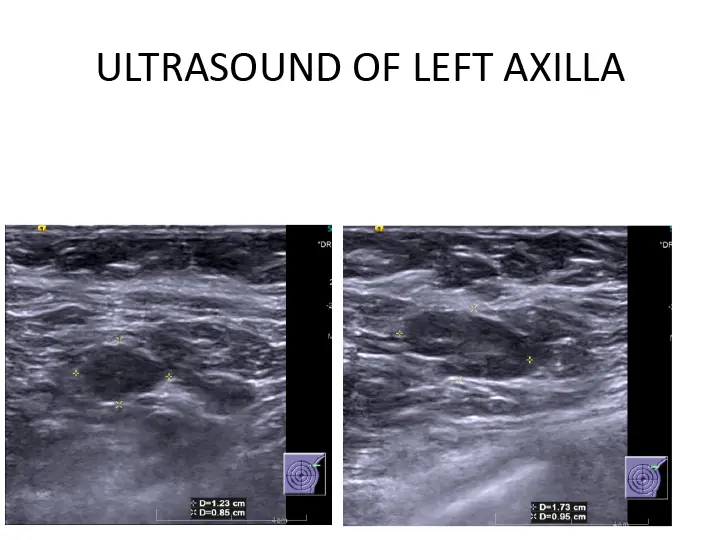
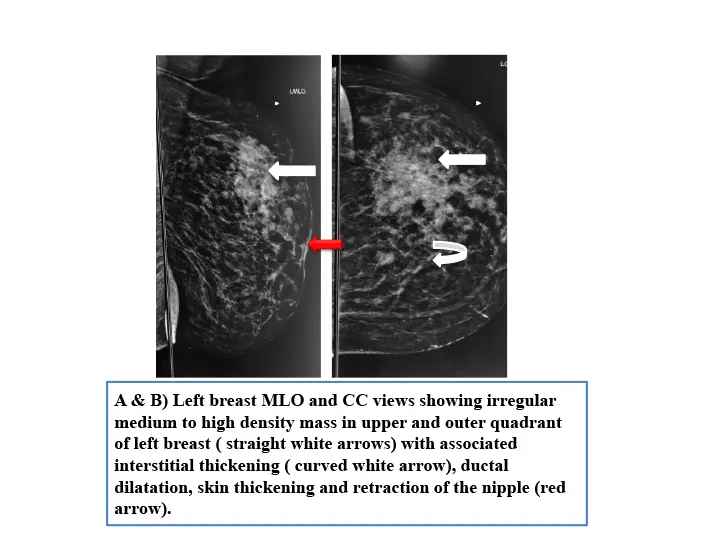
Teaching Case
January 2026
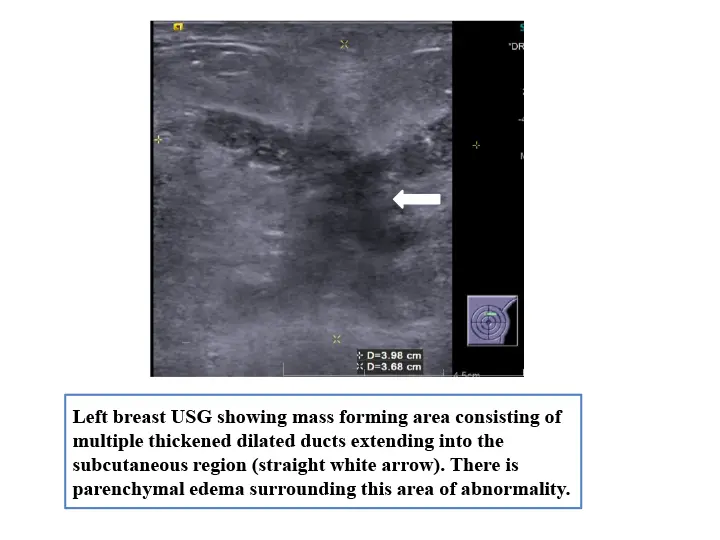
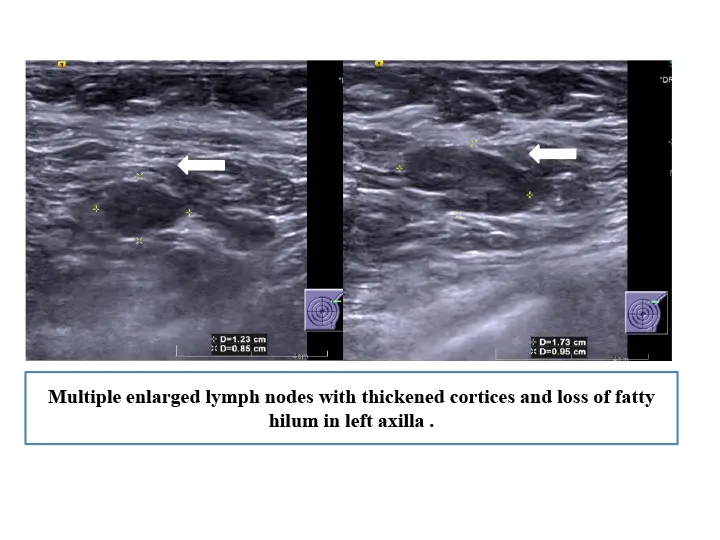
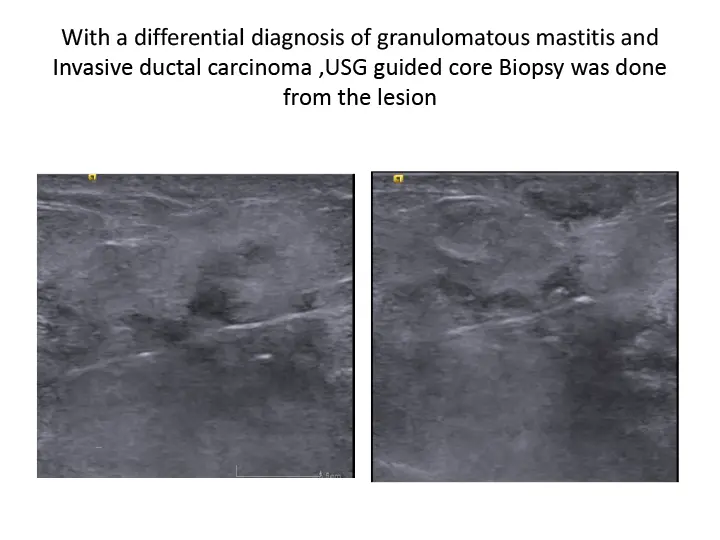
[ Click to Enlarge ]
Join us to get regular opportunities to update your knowledge and skills in breast imaging
Apply Now